Consulting with the communities
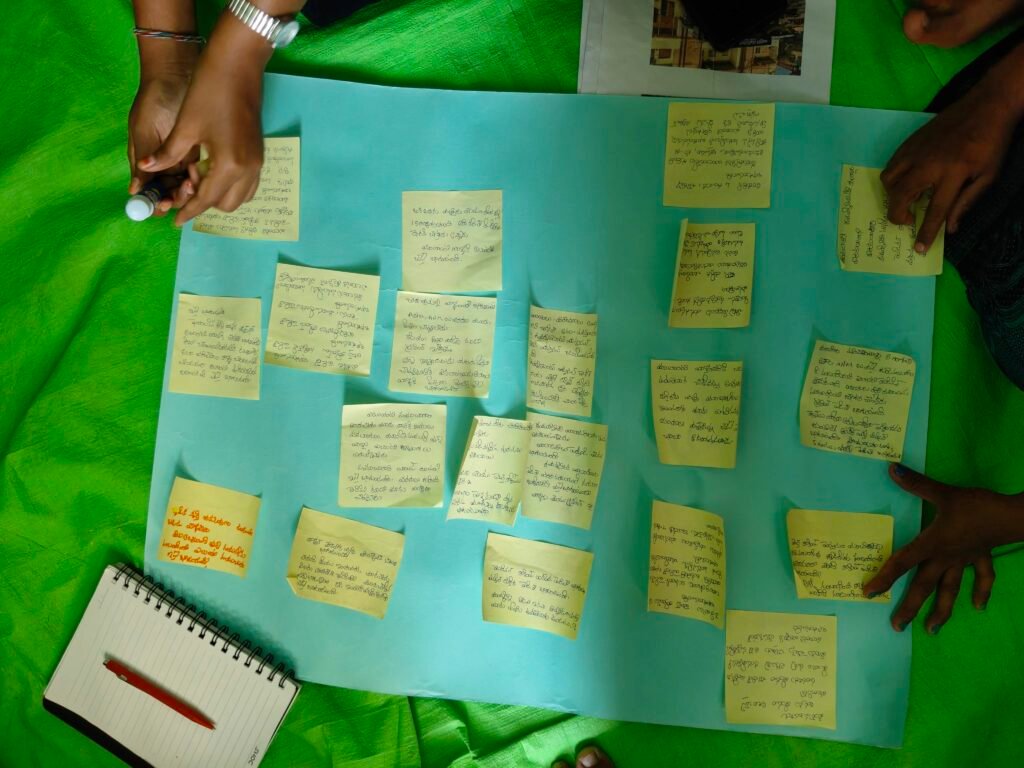
Consulting with the communities “What did you have for tiffin (breakfast)?” This question brings a smile to the faces of the people sitting in for community meetings of the Urban SHADE project. In these meetings that started in February 2026 are conducted in the community, the Vijayawada-Guntur team and the Shimla team discuss the findings and the proposed intervention of the Urban SHADE project. The meetings have been set up in people’s houses within the community which they have generously opened for the Urban SHADE team, despite houses being small and cramped. In Guntur and Vijayawada, the hosts removed the cot from the house to make space for the duration of the meeting. In Shimla too, a friendly person’s house, public spaces such as grounds, or Anganwadi centres or even the lobby of a residential building were used for these meetings. We are grateful to everyone who helped us organise these meetings. The meetings were conducted with different groups from different sites of the settlement- women, old persons, persons with disabilities, outdoor workers and those with chronic illnesses. In Shimla, meetings were also determined by the location- such as upper part of settlement, and the lower parts, and some occupational groups such as municipal sanitation workers. In Vijayawada and Guntur, the team hung relevant photos and distributed some photos among the participants that helped spark discussion among them. There were photos of cracked walls of houses, hospitals, garbage on the road, newspaper headlines of floods, flood warning messages or illustrations depicting heart illness among others. This technique helped a great deal in communicating the findings of the qualitative research including focus group discussions and in-depth interviews, especially since many of the participants were illiterate or semi-literate. Persons who participated in these meetings discussed the garbage in their areas, what happened during the floods, or their experiences in public hospitals or private clinics. Many people who attended the meetings said that they saw the messages sent by the government on flood warnings for the first time. They spoke about how they barely got food or water during the heavy floods in 2024. The community members also suggested their ideas for possible interventions. In Shimla, the team presented an illustrated flow chart with the findings, gaps and the planned intervention activities. The team explained that the qualitative study presented cardiovascular diseases, musculoskeletal problems, skin disease, alcohol and drug addiction as problems facing the community. There are also increased out-of-pocket expenditures due to lack of ambulances and unavailability of medicines in government hospitals. The distance of the hospitals deters people from going there, especially older persons who are unable to walk up to main road, often leading to them missing out on follow-ups. Both informal settlements in Shimla do not have functional Primary health centres. Pregnant women and children have to go to hospitals further away to get basic check-up or immunisation. People reflected on how they are unable to sleep when during heavy rains. While they do get flood messages, they have no idea what action should be taken. The team also presented a general lack of awareness about the diseases caused due to extreme rainfall, and suggested interventions. These meetings helped validate the findings and also get buy-in from the community for the intervention activities still being planned. In Andhra Pradesh the team includes researchers Pavani Pendyala and Hemanth Chandu, field coordinator Satyanarayanamma Methukulla and community co-researchers Dasari Madhavi and Maddela Siva Parvathi. In Shimla, the team includes researchers Inayat Singh Kakar, Dr Yetika Dolker, and field coordinator, Sahil Kumar.




